.png)
Early Orthodontics
Intervening early allows us to address myofunctional imbalances, poor oral habits, improper or asymmetric development, among other clinical variables that influence the growth and development of the middle and lower thirds of the face and ultimately the eruption and alignment of the permanent teeth. By correcting issues early and optimizing ongoing growth and guiding permanent teeth into proper placement, we can facilitate ideal esthetics and function via a gentler approach that will be stable for a lifetime.

Early Interceptive Orthodontics via Habit Optimization & Guided Growth & Development
Early interventional orthodontics via guided growth and development in children as young as 2-3 years old is the superior method of orthodontic treatment and the accepted standard of care in many countries that are motivated to achieve the most stable and best clinical results for their populations (e.g. the Netherlands, Italy, Japan, Australia, New Zealand, Germany, Canada, among many others). This approach allows a patient to achieve a functionally- and esthetically- optimized smile that is stable for a lifetime without use of a permanent retainer (or as many parents from the 80's know, the permanent metal bar glued to the back of their teeth).
"Traditional orthodontics" that typically includes waiting until a patient has reached puberty and the majority of the permanent teeth have erupted is such a dinosaur approach; it is the epitome of "sick care" instead of "health care" in that it leaves a patient at high risk for compromised results including TMJ pain or dysfunction, sleep apnea, gummy smile, diminished esthetics, removal of healthy tissue and teeth to finalize the case, more force needed to move the teeth, and high likelihood for relapse if not permanently retained.
The benefits of early intervention are many, but to name a few:
-
Guided eruption, early interventional orthodontics is the only therapeutic approach that can nearly guarantee a perfect outcome (pending patient compliance with recommended therapy and that no genetic abnormalities exist in the patient pre-treatment); this includes ideal TMJ position and function, tongue posture, arch width and length, esthetics, OJ/OB, and predictable retention
-
Addressing hard and soft tissue issues early when they're easier to treat since these issues tend to get worse with age and become harder to treat
-
Leverage the many "growth spurts" a child experiences as they are developing to achieve desired results, as opposed to applying unnatural forces at puberty when growth is near complete to achieve similar results
-
Gentler forces can be applied because length of time in treatment can be extended
-
Once the permanent teeth are guided into proper alignment, the PDL fibers that attach the teeth to the bone so that a child's own body becomes a natural "retainer" of the targetted position
-
More hygienic in that the majority of treatment (if not all) can be performed with removable appliance therapy, making it easier to brush, floss, and prevent gum disease and cavities
-
System uses more biocompatible materials, thus decreasing the risk of allergic reactions or tissue inflammation
-
Less frequent dental clinic visits - instead of going into the office 1x/mo for 2-3 years of total care that is common with treatment that includes metal braces around puberty, patients who start early can be seen at cleaning visits and for virtual visits to manage progress
-
Remote management, ongoing progress even when traveling - patients who may spend extended periods of time away from the dental clinic can have ongoing management of the case and replacement of appliances mailed directly to them in periods of time when they cannot come into the clinic
For patients who are candidates for this type of treatment, it is important that the parents understand WHY this is the case and HOW the system works. So let's get into the details...

Habit Correction & Optimization
When talking to my patient parents, I often use the analogy of river rocks: rocks are hard, but overtime, the constant movement of the river will change their shape. A child's growing body is very similar: teeth and bone are hard, but overtime, soft tissue such as cheeks, tongue, and lips can drastically alter the position of these hard tissues. And these soft tissues, or "the river", can either be influencing and guiding the hard tissues in the "right"/preferred direction, or they can drastically diverting them into the wrong position. If a child shows any signs or symptoms of these dysfunctions, then we can intervene early to correct them and put them on the right path to ideal growth and development.
First, it is important for parents to understand that malocclusion (or misaligned teeth and poorly formed jaws) is a modern day disease. Renowned dentist and nutrition-enthusiast Dr. Weston Price documented his observations when evaluating the development of the oral anatomy of thousands of patients that could be divided into two main groups:
-
Native and aborigine populations that lived off the land in a more prehistoric, hunter-gatherer lifestyle, completely isolated from modern advancements associated with developed civilizations
-
Modern society in port towns and big cities that leveraged the benefits of organized agriculture and trade
What he found was astonishing. Those from the native populations who, despite no knowledge of or access to dental care, developed well aligned and healthy jaws with broad arches of straight teeth free of cavities and gum disease. And those from the developed populations who had access to dental care but also had diets rich in processed and sugary foods and a very different lifestyle, they quickly presented with cavities, gum disease, crowded teeth, and malformed jaws. And the conditions worsened with each exposed generation.



This is why I encourage all families for early screening and evaluation. Ideally, a patient would present with perfect conditions for the following: (1) Genetics, (2) Delivery, (3) Breastfeeding, (4) Nutrition, (5) Environment, and (6) Habits.
But in most cases, there's no way a child presents with all of these conditions being "perfect." I'm not unrealistic. And I'm not into "parent-shaming". We all are doing the best we can with the variables we have to manage. My intention is to help educate parents, identify concerns, and guide families to make choices that allow the child to be in peak health and live life at their fullest potential. More on variables 1-5 later, let's focus on variable #6 "Habits" first.
Swallowing
A child swallows 2x/min during the day, and 1x/min at night. That's approximately 2,160 swallows per 24 hr; over 15,000 swallows per week; nearly 800,000 per year; and about 4.7 million swallows before the age of 6, before any of the permanent teeth even begin to erupt into the mouth. If these are all proper swallows (with the tongue in the roof of the mouth and then pushing up and back when swallowing and the lips sealed upon rest with the teeth slightly apart), then all of these swallows has the ability to shape the dental arches and help create plenty of room for the permanent teeth to erupt into proper alignment.
However, if the swallows are dysfunctional, asymmetric, or problematic in any other way, then it can have a dramatic impact on the position of the jaws, narrowing of the arches, and can lead to a crossbite, severe crowding, or excess spacing when the permanent teeth do begin to erupt. Not to mention, this can have big implications in speech development and esthetics, both of which can cause issues with self esteem for a growing child.
There are many things that can impact a proper swallow, including, but not limited to:
-
Severe tongue or lip tie that restricts range of motion
-
Prolonged pacifier use (beyond 6 months of age)
-
Thumb sucking (or any sucking habit, fingers, blanket, toy)
-
Minimal or no breastfeeding

The impact of a prolonged pacifier or sucking habit can lead to an anterior open bite, excess spacing, and a posterior crossbite.

A chronic tongue thrust can cause an anterior open bite, compromised esthetics and function, crowding, and speech issues.
Breathing
The respiratory rate of a baby is between 30-60 breaths per minute, and gradually as a child grows, their respiratory rate decreases to 18-24 breaths/min for the average 6 year old, and 15-21 breaths/min for the average 14 year old. If a child is breathing through their nose during the day and at night, it is a good indication that the upper airway anatomy is balanced and the child is breathing in a healthy and stable way. However, if a child is breathing through their mouth at any time during the day or at night, this can have major cascading effects on the development of the oral and maxillofacial anatomy as well as on whole-body health. Watch the video below for a better visualization:
Unlike mouth breathing, nasal breathing ensure proper humidification and filtration. Prolonged mouth breathing has been linked to severely compromised sleep and increased whole-body inflammation, not just poor dental outcomes. For more, we recommend reading James Nestor's Breath.
Sleep
The National Sleep Foundation Recommended Sleep Times:
Toddles (1-2 Years): 11-14 Hours
Preschoolers (3-5 Years): 10-13 Hours
School Aged Children (6-13 Years): 9-11 hours
Teenagers (14-17 Years): 8-9 Hours
Healthy sleep is for the appropriate length of time, breathing through the nose, staying relatively still throughout the night, and waking up refreshed, in a good mood in the morning. It is not healthy for a child to snore or have audible breathing, to toss and turn, to run hot or experience night sweats, to experience prolonged bedwetting, to have recurrent episodes of night terrors or nightmares, or to wake up consistently with mood volatility or other dysfunctional behaviors. While it may be "normal", in that these dysfunctional ways of life have become increasingly more common, that does not mean it is "healthy". Just like smoking cigarettes used to be "normal", it didn't make it "healthy"; or another analogy I often use when explaining this dysfunction to parents... just because it is technically "normal" to be overweight in the US with over 2/3 of the adult population being over their optimal weight, this does not mean that this is "healthy".
Sleep impacts the neurological, cardiovascular, endocrine, and immunologic systems in the body. When these systems are compromised, they have cascading effects on the whole body including the development oral anatomy.
Nutrition & Hydration
A lifestyle that includes a diet rich in colorful fruits and vegetables, organic proteins and fats, and sufficient clean water is one that supports happy and healthy growth. The ingredients of these foods are normally one word or at least a short list of easily recognizable items.
Inflammatory, unhealthy choices include heavily processed foods that are fried or have a lot of ingredients on the back of the bag that you don't recognize nor can pronounce and sugary items, and unless you are drinking fresh pressed celery or beet juice in the morning, there is little to no nutritional benefit to off-the-shelf juices. In fact, most juices and sports drinks just leveraging the benefits of good marketing to make their products appear healthy when they're really no better than the average soda.
When parents explain to me that their child "only eats white foods" or "has a sweet tooth" or "won't drink water unless it's sweetened", I empathize with the struggle. And then I explain to them what has happened to their child on a neurobiological level.

Research shows that sugar is more addictive than cocaine.
So basically, their kid is an addict and has developed a habit that drastically impacts their neural pathways at a time when their brains are still actively growing and developing. (Read the entire study here)
So while it is uncomfortable to think about and may sound extreme, a child who "has a sweet tooth" is actually an addict. And breaking this habit can be very challenging. But a diet with unhealthy foods, both sugary and heavily processed, can drastically compromise the overall health and wellbeing of a child.
Additionally, gnawing on crispy vegetables and raw fruits and grinding up tough meats has been demonstrated to have mechanical benefits to the development of the muscles and bones of the jaw. Add on top of that the density of nutrition in these foods that contain Vit D, Vit C, Zinc, Magnesium, among others are critical in balanced.
As hard as it is to say "no" to sugar when it is so widely available at schools, at birthday parties, and in our homes, I encourage families to make this change now because it is good for the whole family, and it helps build good habits for a lifetime. Not to mention, a child on a more balanced, anti-inflammatory diet is one that is more likely to sleep and breathe better and to have better behavior and comply with recommended therapies moving forward.
How do we fix these habits?
Each child is different because the root causes of their poor habits are different. After a comprehensive evaluation, I identify all contributing risk factors and then in collaboration with the parents and child, we prioritize a list of actionable items to improve these areas of concern. This may include but is not limited to:
-
Modifications to diet and hydration habits
-
Use of over-the-counter remedies to support nasal breathing and improve sleep
-
Implementation of myofunctional exercises to correct tongue and lip function
-
Inclusion of intra-oral appliance therapy (dental appliances) to correct issues
-
Referral to other healthcare specialists for ongoing evaluation and treatment as needed including otorhinolaryngologists (ENTs), pediatricians, sleep physicians, myofunctional therapists, speech therapists, nutritionists, among others
Remember: the earlier we screen, the easier it can be to correct these habits and the more time we have to course correct towards optimal growth and development. I see children as young as infants to help educate parents BEFORE the habits start and/or to evaluate for any malformation that can be corrected early. But there is no "too early" when it comes to evaluating and discussing these types of clinical conditions. And we have to make sure these habits are corrected as we consider moving teeth.

Guided Eruption
So there are two analogies I like to use to explain this idea to parents. One is working with wet clay and how you can easily mold it into any shape that you desire. And if unfamiliar with clay, I ask a parent if they were aware of square watermelons. Basically, the proven practice where you can change the shape of a fruit or a vegetable (or most any growing plant for that matter) if you guide the shape into which it can grow.
Children are very much like wet clay or a growing watermelon.
Ideally, once we have corrected the poor oral habits listed above (or in parallel to that, depending on the age of the child and severity of the case), then we can start guiding the teeth into proper place as the child continues to grow.
How do we know this to be true?

First off, the shape of the human skull and the different components of it have not changed drastically over the last 100 years since we started very meticulously measuring all aspects of the human body. But based on decades and decades or patient records and extensive research from orthodontic and pediatric dental graduate programs, we know with a great level of certainty exactly how and where the head (and jaws and teeth) should grow to end up with an ideal clinical outcome.

The growth of the skull and the jaws is just not that complicated.
There is a constant pattern of growth from ages 2 until puberty. What can make it complex is when different variables (listed above) interfere with or negatively influence this natural progression, and then we have to correct improper growth, reposition the jaws, and move misaligned teeth. Otherwise, a patient is at risk for severe malocclusion, which can mean poor function, poor esthetics, pain, and diminished overall health.
And how are kids like the wet clay or the square watermelon?
I like to use this series of panoramic x-rays of patients at different developmental ages to explain this idea. If you look at the circled teeth in the image on the far left, these are the permanent premolars of an average 7-8 year old. These teeth are just "buds", or just the crowns of the teeth without roots. As you track the progress of these teeth from left to right, you will see that as these permanent teeth push the baby teeth out of the mouth (the process of the baby teeth getting loose and falling out), we see the roots begin to form. And it is only once the permanent teeth are fully erupted and biting against the teeth in the opposite arch do we see the roots have fully formed.
As the teeth are erupting and as the child has more time in growth and development, we can guide the shapes of their arches and the position of their teeth more easily. Once the child reaches puberty, the clay hardens, the watermelon is no longer growing, so trying to change it's shape is limited and requires more force.

Because as those roots are fully formed, there are millions of periodontal ligament fibers (PDL fibers) that grow and attach from the jaw bone to the roots of the teeth to hold them securely in place. These fibers are super strong; and they are one of the reasons why so many patients who are treated at puberty or older experience a 90% relapse rate because the fibers have attached and can only be stretched and twisted and will rebound as soon as the ortho appliances are removed unless permanently retained. Add on top of that any poor oral habit (like a dysfunctional swallow or mouth breathing) that was never corrected that can cause relapse of these conditions.
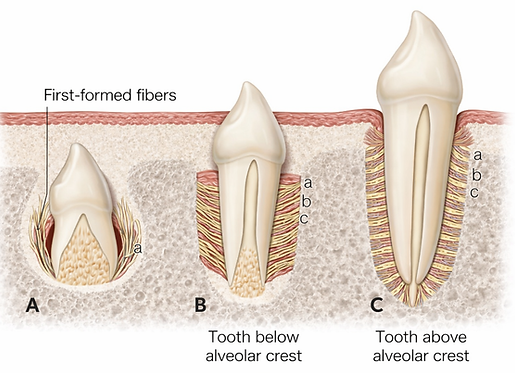

So if we are able to intervene early enough, optimize habits and guide the teeth into proper placement, then as these PDL fibers attach to the teeth, the child's own body becomes their retainer for a lifetime. This is one of the conclusions that can be drawn from a 10-year study out of Finland that showed guided eruption orthodontic therapy to produce the most stable outcomes relative to fixed orthodontics (traditional braces) and no treatment at all.
Example Cases

Case Start: When we started treatment at 8-years-old, this boy presented with a severely narrow upper arch, crowding in the upper anterior associated with premature loss of a front baby tooth, a retrognathic mandible/severe overjet, and poor lip posture. He also presented with symptoms of chronic mouth breathing and a dysfunctional swallow.
18-Month Progress Check: We corrected the habits, realigned the permanent teeth that had already erupted in the wrong position, and then were able to guide the newer permanent teeth into proper alignment. This child will continue with passive care until the remaining permanent teeth erupt, but that will only require him to wear a guiding appliance at night and then routine checks in our clinic every 3-6 months.

Case Start: This 5-year-old boy initially presented with symptoms of sleep-disordered breathing including restless/active sleep, frequent waking, and nightmares, and he had an anterior crossbite (aka an "underbite") that was impeding proper speech and restricting the growth of his maxilla, which was compromising the dental growth as well as the soft tissue profile of the upper lip.
2-Month Progress Check: We corrected the dental issues within 2 months of treatment using intra-oral appliance therapy at night and with 30-60 min of daytime wear. Patient's mother reported a noticeable improvement in speech. Patient is continuing with care, but this is a good example of how quickly a case can improve when we intervene early.

Case Start: This girl started treatment at age 10 and initially presented with excessive spacing and excessive overjet. She also had a history of trauma to a front tooth (as evident in the photos) that is common with patients who have excessive overjet.
18-Month Progress Check: We corrected the anterior alignment, excessive overjet, and excessive overbite. She will remain in passive treatment with nighttime appliance wear only until her remaining permanent teeth erupt into place. Note, the "bumps" on the lip-side of her teeth in the right side progress photos are the bonded attachments necessary for her therapy. We will remove at the completion of treatment.
More cases coming soon...
Frequently Asked Questions
"Oh no! I'm just learning about this and my child is already X years old. Is it too late?"
We hear this all the time. And while it is easiest and best to intervene early, that is not necessarily the case for most of our patients when we first meet them. As a child gets older, the habits can be harder to break; the forces required to move the teeth and jaws must be stronger; and compliance becomes even more important because we have less time with which to work. However, if the patient and the parents are motivated, then we can still achieve an optimal clinical outcome.
How do I know if my child is a candidate for early interventional orthodontic therapy?
Likely the easiest way is to schedule a comprehensive new patient exam in our clinic with Dr. Beth to take records, review the patient's comprehensive history, habits, and environment, and perform a clinical exam. Otherwise, parents can know that their child is likely a candidate if their child isn't a good sleeper, if they have speech issues, if their baby teeth or mixed dentition is crowded or demonstrating excessive spacing, if their jaws don't align properly, and they breathe through their mouths or snore.
How long does treatment take?
Again, each child is a bit different, and we will be able to more specifically predict the length of time in treatment after evaluating your child. "Active treatment" typically means more frequent office visits, closer monitoring of therapy with possible appliance changes; and I try to limit this to 6-9 months for those children who start treatment under the age of 6, and 12-18 months for those children who start treatment after the age of 6.
What happens if we move in the middle of treatment?
So while we do try to manage expectations and anticipate future issues, sometimes life gets in the way, and we need to pivot. Pending the progression of the case, we are sometimes able to finish with tele-visit check ups if the patient is on the tale end of treatment. If the patient is mid-treatment, then we sometimes look for a provider in their new location with a similar philosophy of care and therapeutic approach to whom we can transfer the case. Our ultimate goal is that we want our patients to be healthy and happy, and we really will do all that we can to support that as best as we can regardless of what life throws at them.
Why doesn't every doctor do this?
Well, unfortunately, this isn't the mainstream philosophy of care taught in most US dental schools today. So many doctors are unaware of this approach and/or do not have the training to deliver it. This is absolutely what is taught and the standard of care in other countries. My personal opinion is that the US is so used to a "sick care" type approach to all things health related, that this doesn't align with that philosophy; waiting until puberty and aligning teeth with metal braces and surgery over 2-4 years is the epitome of "wait until something is broken and then fix it". Instead of using the massive amounts of research and historical documentation and advanced technology we have available to us to prevent problems from occurring and/or minimize the issues associated with these problems, we are going with what we have always done. Many US dental offices still use mercury amalgam fillings and recommend fluoride despite better, non-toxic alternatives being available.
It's also my professional opinion that many specialists may prefer the "wait until it's broken and fix it with metal braces" because it is easier to educate and motivate parents to invest in their child's oral health when it is so visibly dysfunctional; and then it is easier to manage a patient when the therapeutic components are glued into the patients mouth, as opposed to relying on compliance with a removable appliance approach. Those specialists are guaranteeing straight teeth, and they can deliver on that; but they are less concerned with how that patient presents 10-20-50 years from now; were they treated with whole body health in mind? Or does this patient with straight teeth have chronic TMJ disorder, sleep apnea, and a litany of other issues because they were treated with this archaic approach. Also, it is much easier to "sell" a very expensive treatment plan to fix a very "broken" smile instead of educating a parent about how a child is showing early signs of dysfunction, and we can prevent it from getting worse with a more affordable approach.
How much does early interventional orthodontic therapy cost?
Each case is unique in the required diagnostics, therapeutics, and ongoing management of the case. Some cases require more advanced screening and diagnostic testing, a mix of different therapeutic systems, and more appointments. That being said, initial phase habit optimization for children ages 2-6 years old can be between $500-1200 for treatment. And once the permanent teeth begin to erupt around or after the age of 6, total therapy is equivalent to comprehensive orthodontic treatment, which can range from $3500-5000 per patient. Many dental insurances have orthodontic coverage that you can inquire about before or after your visit with us to determine your out-of-pocket expense. Additionally, we have various financial options to help make this treatment affordable to all.
If you have more questions or you'd like to book your consult now, please contact us today, and we'd be happy to take care of your smile :)

Call Now
787-665-3630